The Truth About Adult Aquired Flat Foot (AAF)
Overview
There are a few things that can weaken the tendon (and thus move that quitting time a little closer). Women are much more likely than men to develop this condition, and it often takes place around the same time as menopause (around age 60 or so). Steroid use (not always illegal-this may come from having cortisone shots in the area) and smoking may also increase the likelihood for developing PTTD, since steroids tend to weaken tendons. A history of injury in the area, arthritis, or an already flat foot may also serve to push the tendon to declare, That's the last straw! (Silly tendon. As if it even knows what straw is.)
Causes
Flat footedness, most people who develop the condition already have flat feet. With overuse or continuous loading, a change occurs where the arch begins to flatten more than before, with pain and swelling developing on the inside of the ankle. Inadequate support from footwear may occasionally be a contributing factor. Trauma or injury, occasionally this condition may be due to fracture, sprain or direct blow to the tendon. Age, the risk of developing Posterior Tibial Tendon Dysfunction increases with age and research has suggested that middle aged women are more commonly affected. Other possible contributing factors - being overweight and inflammatory arthritis.
Symptoms
Your feet tire easily or become painful with prolonged standing. It's difficult to move your heel or midfoot around, or to stand on your toes. Your foot aches, particularly in the heel or arch area, with swelling along the inner side. Pain in your feet reduces your ability to participate in sports. You've been diagnosed with rheumatoid arthritis; about half of all people with rheumatoid arthritis will develop a progressive flatfoot deformity.
Diagnosis
In the early stages of dysfunction of the posterior tibial tendon, most of the discomfort is located medially along the course of the tendon and the patient reports fatigue and aching on the plantar-medial aspect of the foot and ankle. Swelling is common if the dysfunction is associated with tenosynovitis. As dysfunction of the tendon progresses, maximum pain occurs laterally in the sinus tarsi because of impingement of the fibula against the calcaneus. With increasing deformity, patients report that the shape of the foot changes and that it becomes increasingly difficult to wear shoes. Many patients no longer report pain in the medial part of the foot and ankle after a complete rupture of the posterior tibial tendon has occurred; instead, the pain is located laterally. If a fixed deformity has not occurred, the patient may report that standing or walking with the hindfoot slightly inverted alleviates the lateral impingement and relieves the pain in the lateral part of the foot.
Non surgical Treatment
Nonoperative therapy for posterior tibial tendon dysfunction has been shown to yield 67% good-to-excellent results in 49 patients with stage 2 and 3 deformities. A rigid UCBL orthosis with a medial forefoot post was used in nonobese patients with flexible heel deformities correctible to neutral and less than 10? of forefoot varus. A molded ankle foot orthosis was used in obese patients with fixed deformity and forefoot varus greater than 10?. Average length of orthotic use was 15 months. Four patients ultimately elected to have surgery. The authors concluded that orthotic management is successful in older low-demand patients and that surgical treatment can be reserved for those patients who fail nonoperative treatment.

Surgical Treatment
If cast immobilization fails, surgery is the next alternative. Treatment goals include eliminating pain, halting deformity progression and improving mobility. Subtalar Arthroereisis, 15 minute outpatient procedure, may correct flexible flatfoot deformity (hyperpronation). The procedure involves placing an implant under the ankle joint (sinus tarsi) to prevent abnormal motion. Very little recovery time is required and it is completely reversible if necessary. Ask your Dallas foot doctor for more information about this exciting treatment possibility.
There are a few things that can weaken the tendon (and thus move that quitting time a little closer). Women are much more likely than men to develop this condition, and it often takes place around the same time as menopause (around age 60 or so). Steroid use (not always illegal-this may come from having cortisone shots in the area) and smoking may also increase the likelihood for developing PTTD, since steroids tend to weaken tendons. A history of injury in the area, arthritis, or an already flat foot may also serve to push the tendon to declare, That's the last straw! (Silly tendon. As if it even knows what straw is.)
Causes
Flat footedness, most people who develop the condition already have flat feet. With overuse or continuous loading, a change occurs where the arch begins to flatten more than before, with pain and swelling developing on the inside of the ankle. Inadequate support from footwear may occasionally be a contributing factor. Trauma or injury, occasionally this condition may be due to fracture, sprain or direct blow to the tendon. Age, the risk of developing Posterior Tibial Tendon Dysfunction increases with age and research has suggested that middle aged women are more commonly affected. Other possible contributing factors - being overweight and inflammatory arthritis.
Symptoms
Your feet tire easily or become painful with prolonged standing. It's difficult to move your heel or midfoot around, or to stand on your toes. Your foot aches, particularly in the heel or arch area, with swelling along the inner side. Pain in your feet reduces your ability to participate in sports. You've been diagnosed with rheumatoid arthritis; about half of all people with rheumatoid arthritis will develop a progressive flatfoot deformity.
Diagnosis
In the early stages of dysfunction of the posterior tibial tendon, most of the discomfort is located medially along the course of the tendon and the patient reports fatigue and aching on the plantar-medial aspect of the foot and ankle. Swelling is common if the dysfunction is associated with tenosynovitis. As dysfunction of the tendon progresses, maximum pain occurs laterally in the sinus tarsi because of impingement of the fibula against the calcaneus. With increasing deformity, patients report that the shape of the foot changes and that it becomes increasingly difficult to wear shoes. Many patients no longer report pain in the medial part of the foot and ankle after a complete rupture of the posterior tibial tendon has occurred; instead, the pain is located laterally. If a fixed deformity has not occurred, the patient may report that standing or walking with the hindfoot slightly inverted alleviates the lateral impingement and relieves the pain in the lateral part of the foot.
Non surgical Treatment
Nonoperative therapy for posterior tibial tendon dysfunction has been shown to yield 67% good-to-excellent results in 49 patients with stage 2 and 3 deformities. A rigid UCBL orthosis with a medial forefoot post was used in nonobese patients with flexible heel deformities correctible to neutral and less than 10? of forefoot varus. A molded ankle foot orthosis was used in obese patients with fixed deformity and forefoot varus greater than 10?. Average length of orthotic use was 15 months. Four patients ultimately elected to have surgery. The authors concluded that orthotic management is successful in older low-demand patients and that surgical treatment can be reserved for those patients who fail nonoperative treatment.
Surgical Treatment
If cast immobilization fails, surgery is the next alternative. Treatment goals include eliminating pain, halting deformity progression and improving mobility. Subtalar Arthroereisis, 15 minute outpatient procedure, may correct flexible flatfoot deformity (hyperpronation). The procedure involves placing an implant under the ankle joint (sinus tarsi) to prevent abnormal motion. Very little recovery time is required and it is completely reversible if necessary. Ask your Dallas foot doctor for more information about this exciting treatment possibility.
What's The Main Cause Of Achilles Tendon Pain ?
Overview
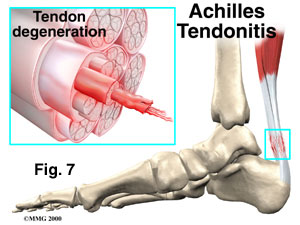 Achilles tendinitis can be a very crippling issue for runners - simply because the pain is enough to discourage loading of the foot. It can also be a tricky condition to treat because the tendon is not as heavily vascularized (i.e. more blood flow) as muscle, and therefore lacks healing potential. It is highly recommended that you see a physical therapist as soon as you experience acute symptoms, so chronic tendonosis (which is longer termed and harder to treat) does not set in.
Achilles tendinitis can be a very crippling issue for runners - simply because the pain is enough to discourage loading of the foot. It can also be a tricky condition to treat because the tendon is not as heavily vascularized (i.e. more blood flow) as muscle, and therefore lacks healing potential. It is highly recommended that you see a physical therapist as soon as you experience acute symptoms, so chronic tendonosis (which is longer termed and harder to treat) does not set in.
Causes
The causes of Achilles tendonitis all appear to be related to excessive stress being transmitted through the tendon. Weak calf muscles, poor ankle range of motion, and excessive pronation have all been connected with the development of Achilles problems.The upshot is that all of these factors, plus training volume and so on, result in damage to the tendon. Much like a bungee cord is made up of tiny strands of rubber aligned together, tendons are comprised of small fiber-like proteins called collagen. Pain in the Achilles tendon is a result of damage to the collagen. Because of this, treatment options should start with ways to address this.
Symptoms
Gradual onset of pain and stiffness over the tendon, which may improve with heat or walking and worsen with strenuous activity. Tenderness of the tendon on palpation. There may also be crepitus and swelling. Pain on active movement of the ankle joint. Ultrasound or MRI may be necessary to differentiate tendonitis from a partial tendon rupture.
Diagnosis
During an examination of the foot and ankle, you doctor will look for the following signs, Achilles tendon swelling or thickening. Bone spurs appearing at the lower part of the tendon at the back of the hell. Pain at the middle or lower area of the Achilles tendon. Limited range of motion of the foot and ankle, and a decreased ability to flex the foot. Your doctor may perform imaging tests, such as X-rays and MRI scans, to make a diagnosis of Achilles tendinitis. X-rays show images of the bones and can help the physician to determine if the Achilles tendon has become hardened, which indicated insertional Achilles tendinitis. MRI scans may not be necessary, but they are important guides if you are recommended to have surgical treatment. An MRI can show the severity of the damage and determine what kind of procedure would be best to address the condition.
Nonsurgical Treatment
Relieving the stress is the first course of action. Treatment involves ice therapy and activity modification to reduce inflamation. Active stretching and strengthening exercises will assist rehabilitation of the gastrocnemius-soleus complex. When placed in a heeled shoe, the patient will immediately notice a difference, compared to flat ground. It is recommended that the patient be fitted with proper shoes & orthotics to control pronation and maintain proper alignment, relieving the stress on the achilles tendon. Tightness in the tendon itself can be helped by an extra heel lift added to the orthotics. The patient can expect a slow recovery over a period of months.

Surgical Treatment
Occasionally, conservative management of Achilles tendon conditions fails. This failure is more common in older male patients and those with longstanding symptoms, those who persist in full training despite symptoms or those who have uncorrected predisposing factors. In these cases, surgery may be indicated. It should be remembered, however, that the rehabilitation program, particularly for severe Achilles tendon injuries, is a slow, lengthy program. Surgery is only indicated when there is failure to progress in the rehabilitation program. Surgery should not be considered unless at least six months of appropriate conservative management has failed to lead to improvement.
Prevention
Do strengthening and stretching exercises to keep calf muscles strong and flexible. Keep your hamstring muscles flexible by stretching. Warm up and stretch adequately before participating in any sports. Always increase the intensity and duration of training gradually. Do not continue an exercise if you experience pain over the tendon. Wear properly fitted running and other sports shoes, including properly fitted arch supports if your feet roll inwards excessively (over-pronate).
Achilles tendinitis can be a very crippling issue for runners - simply because the pain is enough to discourage loading of the foot. It can also be a tricky condition to treat because the tendon is not as heavily vascularized (i.e. more blood flow) as muscle, and therefore lacks healing potential. It is highly recommended that you see a physical therapist as soon as you experience acute symptoms, so chronic tendonosis (which is longer termed and harder to treat) does not set in.
Causes
The causes of Achilles tendonitis all appear to be related to excessive stress being transmitted through the tendon. Weak calf muscles, poor ankle range of motion, and excessive pronation have all been connected with the development of Achilles problems.The upshot is that all of these factors, plus training volume and so on, result in damage to the tendon. Much like a bungee cord is made up of tiny strands of rubber aligned together, tendons are comprised of small fiber-like proteins called collagen. Pain in the Achilles tendon is a result of damage to the collagen. Because of this, treatment options should start with ways to address this.
Symptoms
Gradual onset of pain and stiffness over the tendon, which may improve with heat or walking and worsen with strenuous activity. Tenderness of the tendon on palpation. There may also be crepitus and swelling. Pain on active movement of the ankle joint. Ultrasound or MRI may be necessary to differentiate tendonitis from a partial tendon rupture.
Diagnosis
During an examination of the foot and ankle, you doctor will look for the following signs, Achilles tendon swelling or thickening. Bone spurs appearing at the lower part of the tendon at the back of the hell. Pain at the middle or lower area of the Achilles tendon. Limited range of motion of the foot and ankle, and a decreased ability to flex the foot. Your doctor may perform imaging tests, such as X-rays and MRI scans, to make a diagnosis of Achilles tendinitis. X-rays show images of the bones and can help the physician to determine if the Achilles tendon has become hardened, which indicated insertional Achilles tendinitis. MRI scans may not be necessary, but they are important guides if you are recommended to have surgical treatment. An MRI can show the severity of the damage and determine what kind of procedure would be best to address the condition.
Nonsurgical Treatment
Relieving the stress is the first course of action. Treatment involves ice therapy and activity modification to reduce inflamation. Active stretching and strengthening exercises will assist rehabilitation of the gastrocnemius-soleus complex. When placed in a heeled shoe, the patient will immediately notice a difference, compared to flat ground. It is recommended that the patient be fitted with proper shoes & orthotics to control pronation and maintain proper alignment, relieving the stress on the achilles tendon. Tightness in the tendon itself can be helped by an extra heel lift added to the orthotics. The patient can expect a slow recovery over a period of months.
Surgical Treatment
Occasionally, conservative management of Achilles tendon conditions fails. This failure is more common in older male patients and those with longstanding symptoms, those who persist in full training despite symptoms or those who have uncorrected predisposing factors. In these cases, surgery may be indicated. It should be remembered, however, that the rehabilitation program, particularly for severe Achilles tendon injuries, is a slow, lengthy program. Surgery is only indicated when there is failure to progress in the rehabilitation program. Surgery should not be considered unless at least six months of appropriate conservative management has failed to lead to improvement.
Prevention
Do strengthening and stretching exercises to keep calf muscles strong and flexible. Keep your hamstring muscles flexible by stretching. Warm up and stretch adequately before participating in any sports. Always increase the intensity and duration of training gradually. Do not continue an exercise if you experience pain over the tendon. Wear properly fitted running and other sports shoes, including properly fitted arch supports if your feet roll inwards excessively (over-pronate).
Understanding How To Cope With Diabetic Feet
Persistent unilateral (one -sided) swelling of feet can be a sign of serious damage to the bones and joints of his feet and needs to be shown to a doctor immediately. If the foot wear is worn out at particular place, it is indicative of extra pressure being applied at that area of the foot and needs to be shown to the doctor at the earliest. While traveling, one must not remove his/her footwear and rest the feet on the floor of the vehicle. No amount of drugs/medicines can keep a patient's feet intact unless the patient is wearing properly designed footwear. All foot wear must always be worn with socks. It is necessary to avoid direct contact between the footwear and skin. Socks also help in reducing the damage to the skin of the fore foot. The heel of the foot should be completely supported by FULL HEEL COUNTER. Diabetic neuroischemic foot.

Whether the injury is in the brain, the spinal cord or peripheral nervous system, if the areas that pertain to the foot are affected, then numbness, weakness and paralysis can occur. Foot numbness can be present in disorders such as peripheral arterial disease, hypothyroidism and alcoholism. Nerve damage resulting in foot numbness can also be caused by drugs, toxins, prolonged exposure to cold and pressure from a poorly fitted cast, splint, brace or crutches. Chronic kidney disease, autoimmune disorders, low levels of vitamin B-12 or other dietary deficiencies, human immunodeficiency virus and liver infections are also associated with peripheral neuropathy and foot numbness. Foot numbness is dangerous because you might injure your foot and not know it. In diabetes this is especially hazardous because slow healing can allow small injuries to develop into gangrene, which can lead to amputation. As a result, the skin becomes itchy.
There is in this case, a problem for the diabetic in telling the difference between sharp pain and a more dull pain. Consequently major cuts and wounds often go undetected and diabetic foot ulcers can become problematic. However without effective feedback from the nerves in your foot ot toe, then that adjustment is not adequately made.
Also, the article references studies that show that MRSA increases the cost of treatment and can keep you in the hospital longer. If you do have an open sore, see your health care provider right away. With good hygiene practices and good foot care , you can reduce your risk for infections, including MRSA. Keeping your blood sugar under control can also help by lowering your risk of all foot complications including sores, ulcers and neuropathy. A foot physician must both get comprehensive instruction for that therapy of the various foot problems equally by medical in addition to operative means. This motion-control coach is designed with supreme padding and both utmost stability therefore the stabilization is very good, plus they always keep your foot in right position. Fundamentally the body determines that it takes more assistance inside of the foot.
Check shoes before they are put on the feet to make sure there are no rocks or objects inside of the shoes. Diabetics who have a loss of feeling in the feet may not be able to feel objects inside shoes, even when they are causing harm to the feet. You may have serious foot problems, but feel no pain.
To help improve the current situation and ultimately reduce amputation rates amongst diabetic patients, Diabetes UK is calling on healthcare professionals to ensure everyone with diabetes has their Back Pain feet checked at least once a year; are informed of their risk status; and understand the importance of good foot care and the urgent need to see their GP if they have any signs of a foot attack.
Whether the injury is in the brain, the spinal cord or peripheral nervous system, if the areas that pertain to the foot are affected, then numbness, weakness and paralysis can occur. Foot numbness can be present in disorders such as peripheral arterial disease, hypothyroidism and alcoholism. Nerve damage resulting in foot numbness can also be caused by drugs, toxins, prolonged exposure to cold and pressure from a poorly fitted cast, splint, brace or crutches. Chronic kidney disease, autoimmune disorders, low levels of vitamin B-12 or other dietary deficiencies, human immunodeficiency virus and liver infections are also associated with peripheral neuropathy and foot numbness. Foot numbness is dangerous because you might injure your foot and not know it. In diabetes this is especially hazardous because slow healing can allow small injuries to develop into gangrene, which can lead to amputation. As a result, the skin becomes itchy.
There is in this case, a problem for the diabetic in telling the difference between sharp pain and a more dull pain. Consequently major cuts and wounds often go undetected and diabetic foot ulcers can become problematic. However without effective feedback from the nerves in your foot ot toe, then that adjustment is not adequately made.
Also, the article references studies that show that MRSA increases the cost of treatment and can keep you in the hospital longer. If you do have an open sore, see your health care provider right away. With good hygiene practices and good foot care , you can reduce your risk for infections, including MRSA. Keeping your blood sugar under control can also help by lowering your risk of all foot complications including sores, ulcers and neuropathy. A foot physician must both get comprehensive instruction for that therapy of the various foot problems equally by medical in addition to operative means. This motion-control coach is designed with supreme padding and both utmost stability therefore the stabilization is very good, plus they always keep your foot in right position. Fundamentally the body determines that it takes more assistance inside of the foot.
Check shoes before they are put on the feet to make sure there are no rocks or objects inside of the shoes. Diabetics who have a loss of feeling in the feet may not be able to feel objects inside shoes, even when they are causing harm to the feet. You may have serious foot problems, but feel no pain.
To help improve the current situation and ultimately reduce amputation rates amongst diabetic patients, Diabetes UK is calling on healthcare professionals to ensure everyone with diabetes has their Back Pain feet checked at least once a year; are informed of their risk status; and understand the importance of good foot care and the urgent need to see their GP if they have any signs of a foot attack.
What Is Painful Heel

Overview
Plantar Fasciitis is a common athletic injury of the foot. While runners are most likely to suffer from plantar fasciitis, any athlete whose sport involves intensive use of the feet may be vulnerable. The risk of plantar fasciitis increases in athletes who have a particularly high arch, or uneven leg length, though improper biomechanics of the athlete’s gait and simple overuse tend to be the primary culprits. If you suffer from plantar fasciitis or are seeking to prevent its occurrence it is important to follow the information in this article. In addition, adding a few simple stretches to your fitness program will also help.
Causes
Currently no single factor has been reliably identified as contributing to the development of plantar fasciitis. The two risk factors with the most support from current research. Decreased ankle dorsiflexion. Increased Body Mass Index (BMI) in non-athletic populations. These factors are related in that both lead to increased strain on the arch, both lead to increased compression on the heel. When dorsiflexion range of motion (ankle flexibility) is lacking, the body compensates by increasing movement of the arch. In this way, decreased ankle dorsiflexion influences pronation and places strain on the underside of the foot. Similarly, having a high BMI causes strain because it places a load on the foot that may be in excess of what the foot can support. As mentioned earlier, overpronation is thought to be a contributing factor, but studies on this have so far produced mixed results. The second way these factors relate to each other is in the way people stand. A lack of ankle flexibility and a high BMI can both cause increased pressure on the heel in standing. Keeping weight on the heels causes compression under the heel. But it also means the muscles and ligaments in the arch are not being used to balance your body weight. Lack of use, I suspect, is a greater danger than overuse. Looking beyond these potential contributors to heel pain though, there is one major factor that overshadows them all-the way footwear alters the normal function of the foot.
Symptoms
You'll typically first notice early plantar fasciitis pain under your heel or in your foot arch in the morning or after resting. Your heel pain will be worse with the first steps and improves with activity as it warms up. As plantar fasciitis deteriorates, the pain will be present more often. You can determine what stage your are in using the following guidelines. No Heel Pain, Normal! Heel pain after exercise. Heel pain before and after exercise. Heel pain before, during and after exercise. Heel pain all the time. Including at rest! This symptom progression is consistent with the four stages of a typical overuse injury. Ultimately, further trauma and delayed healing will result in the formation of calcium (bone) within the plantar fascia. When this occurs adjacent to the heel bone it is known as heel spurs, which have a longer rehabilitation period.
Diagnosis
A thorough subjective and objective examination from a physiotherapist is usually sufficient to diagnose plantar fasciitis. Occasionally, further investigations such as an X-ray, ultrasound or MRI may be required to assist with diagnosis and assess the severity of the condition.
Non Surgical Treatment
A steroid (cortisone) injection is sometimes tried if your pain remains bad despite the above 'conservative' measures. It may relieve the pain in some people for several weeks but does not always cure the problem. It is not always successful and may be sore to have done. Steroids work by reducing inflammation. Sometimes two or three injections are tried over a period of weeks if the first is not successful. Steroid injections do carry some risks, including (rarely) tearing (rupture) of the plantar fascia. Extracorporeal shock-wave therapy. In extracorporeal shock-wave therapy, a machine is used to deliver high-energy sound waves through your skin to the painful area on your foot. It is not known exactly how it works, but it is thought that it might stimulate healing of your plantar fascia. One or more sessions of treatment may be needed. This procedure appears to be safe but it is uncertain how well it works. This is mostly because of a lack of large, well-designed clinical trials. You should have a full discussion with your doctor about the potential benefits and risks. In studies, most people who have had extracorporeal shock-wave therapy have little in the way of problems. However, possible problems that can occur include pain during treatment, skin reddening, and swelling of your foot or bruising. Another theoretical problem could include the condition getting worse because of rupture of your plantar fascia or damage to the tissues in your foot. More research into extracorporeal shock-wave therapy for plantar fasciitis is needed. Other treatments. Various studies and trials have been carried out looking at other possible treatments for plantar fasciitis. Such treatments include injection with botulinum toxin and treatment of the plantar fascia with radiotherapy. These treatments may not be widely available. Some people benefit from wearing a special splint overnight to keep their Achilles tendon and plantar fascia slightly stretched. The aim is to prevent the plantar fascia from tightening up overnight. In very difficult cases, sometimes a plaster cast or a removable walking brace is put on the lower leg. This provides rest, protection, cushioning and slight stretching of the plantar fascia and Achilles tendon. However, the evidence for the use of splint treatment of plantar fasciitis is limited.

Surgical Treatment
When more-conservative measures aren't working, your doctor might recommend steroid shots. Injecting a type of steroid medication into the tender area can provide temporary pain relief. Multiple injections aren't recommended because they can weaken your plantar fascia and possibly cause it to rupture, as well as shrink the fat pad covering your heel bone. Extracorporeal shock wave therapy. In this procedure, sound waves are directed at the area of heel pain to stimulate healing. It's usually used for chronic plantar fasciitis that hasn't responded to more-conservative treatments. This procedure may cause bruises, swelling, pain, numbness or tingling and has not been shown to be consistently effective. Surgery. Few people need surgery to detach the plantar fascia from the heel bone. It's generally an option only when the pain is severe and all else fails. Side effects include a weakening of the arch in your foot.
What Exactly Will Cause Heel Pain
Overview
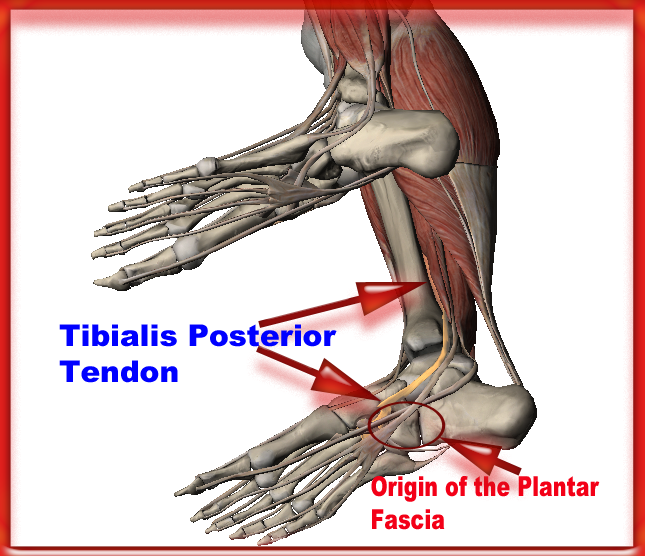
The plantar fascia is a thickened fibrous aponeurosis that originates from the medial tubercle of the calcaneus and runs forward to form the longitudinal foot arch. The function of the plantar fascia is to provide static support of the longitudinal arch and dynamic shock absorption. Individuals with pes planus (low arches or flat feet) or pes cavus (high arches) are at increased risk for developing plantar fasciitis.
Causes
Far and away the most common cause of plantar fasciitis in an athlete is faulty biomechanics of the foot or leg. Faulty biomechanics causes the foot to sustain increased or prolonged stresses over and above those of routine ground contacts. Throughout the phase of ground contact, the foot assumes several mechanical positions to dissipate shock while at the same time placing the foot in the best position to deliver ground forces. With heel landing the foot is supinated (ankle rolled out). At mid-stance the foot is pronated (ankle rolled in). The foot is supinated again with toe-off. The supination of the foot at heel strike and toe-off makes the foot a rigid lever. At heel strike the shock of ground contact is transferred to the powerful quads. During toe-off forward motion is created by contraction of the gastroc complex plantar flexing the rigid lever of the foot pushing the body forward.
Symptoms
The major complaint of those with plantar fasciitis is pain and stiffness in the bottom of the heel. This develops gradually over time. It usually affects just one foot, but can affect both feet. Some people describe the pain as dull, while others experience a sharp pain, and some feel a burning or ache on the bottom of the foot extending outward from the heel. The pain is usually worse in the morning when you take your first steps out of bed, or if you’ve been sitting or lying down for a while. Climbing stairs can be very difficult due to the heel stiffness. After prolonged activity, the pain can flare-up due to increased inflammation. Pain is not usually felt during the activity, but rather just after stopping.
Diagnosis
X-rays are a commonly used diagnostic imaging technique to rule out the possibility of a bone spur as a cause of your heel pain. A bone spur, if it is present in this location, is probably not the cause of your pain, but it is evidence that your plantar fascia has been exerting excessive force on your heel bone. X-ray images can also help determine if you have arthritis or whether other, more rare problems, stress fractures, bone tumors-are contributing to your heel pain.
Non Surgical Treatment
There are a number of treatments that can help relieve heel pain and speed up your recovery. These include resting your heel, try to avoid walking long distances and standing for long periods, regular stretching, stretching your calf muscles and plantar fascia, pain relief, using an icepack on the affected heel and taking painkillers, such as non-steroidal anti-inflammatory drugs (NSAIDs) wearing good-fitting shoes that support and cushion your foot, running shoes are particularly useful, using supportive devices such as orthoses (rigid supports that are put inside the shoe) or strapping. Around four out of five cases of heel pain resolve within a year. However, having heel pain for this length of time can often be frustrating and painful. In around one in 20 cases, the above treatments are not enough, and surgery may be recommended to release the plantar fascia.

Surgical Treatment
Most patients have good results from surgery. However, because surgery can result in chronic pain and dissatisfaction, it is recommended only after all nonsurgical measures have been exhausted. The most common complications of release surgery include incomplete relief of pain and nerve damage.
What Is Plantar Fasciitis
Overview
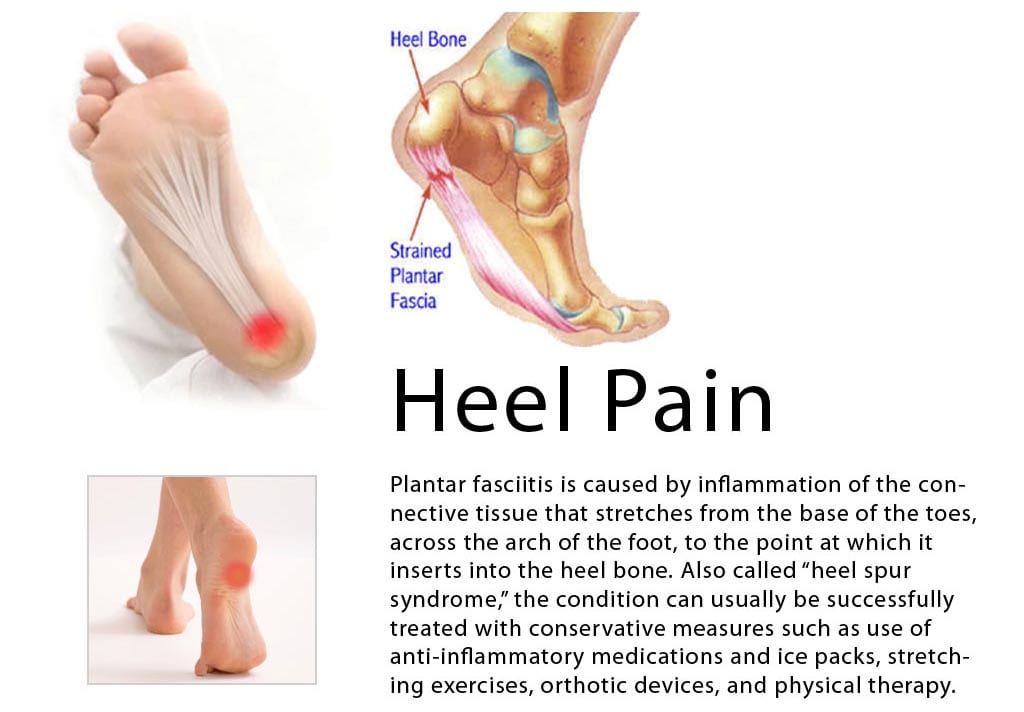
Plantar fasciitis is a poorly understood condition. There is little consensus among medical professionals about what causes the problem, and no treatments have been reliably proven to treat it. A number of theories exists for why plantar fasciitis develops, but the ineffectiveness of conventional treatments suggests something is missing. The plantar fascia is a band of connective tissue that runs along the underside of the foot from the heel to the toes. The fascia helps maintain the integrity of the arch, provides shock absorption, and plays an important role in the normal mechanical function of the foot.
Causes
Plantar Fasciitis is frequently cited as the number one cause of heel pain. The condition affects both children and adults. Children typically outgrow the problem, but affected adults may experience recurring symptoms over the course of many months or years. The syndrome afflicts both highly active and sedentary individuals. Typically, Plantar Fasciitis results from a combination of causes, including, pronation, a condition in which the plantar fascia doesn't transfer weight evenly from the heel to the ball of the foot when you walk. Overuse of the feet without adequate periods of rest. High arches, flat feet or tightness in the Achilles' tendon at the back of the heel. Obesity. Working conditions that involve long hours spent standing or lifting heavy objects. Worn or ill-fitting footwear. The normal aging process, which can result in a loss of soft tissue elasticity. Physical trauma to the foot, as in the case of taking a fall or being involved in a car accident.
Symptoms
The symptoms of plantar fasciitis include pain in the bottom of your foot, especially at the front or centre of the heel bone, pain that is worse when first rising in the morning (called "first-step pain"), when first standing up after any long period of sitting, or after increased levels of activity especially in non-supportive shoes. Seek medical advice about plantar fasciitis if you have heel pain or pain in the bottom of your foot, especially when you get up in the morning, that does not respond to treatment or if there is redness or bruising in the heel.
Diagnosis
Your doctor will check your feet and watch you stand and walk. He or she will also ask questions about your past health, including what illnesses or injuries you have had. Your symptoms, such as where the pain is and what time of day your foot hurts most. How active you are and what types of physical activity you do. Your doctor may take an X-ray of your foot if he or she suspects a problem with the bones of your foot, such as a stress fracture.
Non Surgical Treatment
Stabilize the foot by using uniquely placed wedges, deep heel cups, and "posts" (stabilizers). When the foot is stabilized, it is brought back to a neutral or normal alignment. When the foot is in its normal alignment, pronation and supination are reduced or completely corrected, and the abnormal pull on the Plantar Fascia is alleviated. This will allow the Plantar Fascia to begin to heal. When healing occurs, the pain and inflammation gradually subside. Provide the specific amount of arch support that your foot requires. Our custom-made orthotics support not only the arch as a whole, but each individual bone and joint that forms the arch. Whether your arch is flat or abnormally high, our custom-made orthotics will provide the support that you need. When the arch is properly supported, the Plantar Fascia is protected and healing can begin. Aid in shock absorption. The primary shock absorbers of our feet, and therefore our body, are the Plantar Fascia and the arch. To aid these structures, we construct our custom-made orthotics so that they provide semi-flexible support to the arch by "giving" to absorb the shock of each step, rather than our foot absorbing the shock (our orthotics act in the same way a shock absorber does on an automobile). When your weight is removed from the orthotic, the arch returns to its original height since the material we use has a built-in "memory." This action will help to keep the Plantar Fascia and arch healthy and pain free. Cushion the heel. Our custom-made orthotics use thin, cushiony, durable, materials to cushion and protect the heel. This helps to alleviate painful heels.
Surgical Treatment
Surgery for plantar fasciitis can be very successful in the right patients. While there are potential complications, about 70-80% of patients will find relief after plantar fascia release surgery. This may not be perfect, but if plantar fasciitis has been slowing you down for a year or more, it may well be worth these potential risks of surgery. New surgical techniques allow surgery to release the plantar fascia to be performed through small incisions using a tiny camera to locate and cut the plantar fascia. This procedure is called an endoscopic plantar fascia release. Some surgeons are concerned that the endoscopic plantar fascia release procedure increases the risk of damage to the small nerves of the foot. While there is no definitive answer that this endoscopic plantar fascia release is better or worse than a traditional plantar fascia release, most surgeons still prefer the traditional approach.
What Leads To Heel Discomfort To Flare Up

Overview
The plantar fascia is made up of 3 distinct parts: the medial, central, and lateral bands. The central plantar fascia is the thickest and strongest section, and this segment is also the most likely to be involved with plantar fasciitis. In normal circumstances, the plantar fascia acts like a windlass mechanism to provide tension and support through the arch. It functions as a tension bridge in the foot, providing both static support and dynamic shock absorption.
Causes
Plantar fasciitis is caused by straining the ligament that supports your arch. Repeated strain can cause tiny tears in the ligament. These can lead to pain and swelling. This is more likely to happen if your feet roll inward too much when you walk, you have high arches or flat feet. You walk, stand, or run for long periods of time, especially on hard surfaces. You are overweight. You wear shoes that don't fit well or are worn out. You have tight Achilles tendons or calf muscles.
Symptoms
The symptoms of plantar fasciitis include pain in the bottom of your foot, especially at the front or centre of the heel bone, pain that is worse when first rising in the morning (called "first-step pain"), when first standing up after any long period of sitting, or after increased levels of activity especially in non-supportive shoes. Seek medical advice about plantar fasciitis if you have heel pain or pain in the bottom of your foot, especially when you get up in the morning, that does not respond to treatment or if there is redness or bruising in the heel.
Diagnosis
Your doctor will check your feet and watch you stand and walk. He or she will also ask questions about your past health, including what illnesses or injuries you have had. Your symptoms, such as where the pain is and what time of day your foot hurts most. How active you are and what types of physical activity you do. Your doctor may take an X-ray of your foot if he or she suspects a problem with the bones of your foot, such as a stress fracture.
Non Surgical Treatment
Biomechanical plantar fasciitis can be easily reduced by correcting misalignment of the feet. Wearing orthopedic shoes for plantar fasciitis and orthotic inserts is an easy, effective method of naturally realigning the foot. Worn consistently from first thing in the morning to last thing at night, orthotic support can reduce and sometimes eliminate plantar fasciitis. Biomechanical plantar fasciitis can be easily reduced by correcting misalignment of the feet. Wearing orthopedic shoes for plantar fasciitis and orthotic inserts is an easy, effective method of naturally realigning the foot. Worn consistently from first thing in the morning to last thing at night, orthotic support can reduce and sometimes eliminate plantar fasciitis. Preserve Your Arch with Strengthening Exercises. While seated and barefoot, squeeze your foot as if you have a small marble under the ball of your foot. If you just happen to have a few marbles handy, you can actually practice picking them up between your toes and ball of your foot - and then set them down again. This stretches and helps strengthen the muscles that run under metatarsals (the longest bones in the foot which create its arched shape). Slowly Increase Physical Activity. If you're a runner, a tried and true method of preventing over-use injuries is to only increase your mileage by 10% weekly, max. If you’re new to a walking program, the same caution should be exercised. Ice and Rest. After mild stretching, use a frozen water bottle to roll under the arch of your foot for 10-20 minutes. It may be possible to make an active recovery by wearing Orthaheel Technology to keep your feet naturally aligned, therefore reducing strain on the plantar fascia, while moving throughout your day.

Surgical Treatment
Plantar fasciotomy is often considered after conservative treatment has failed to resolve the issue after six months and is viewed as a last resort. Minimally invasive and endoscopic approaches to plantar fasciotomy exist but require a specialist who is familiar with certain equipment. Heel spur removal during plantar fasciotomy has not been found to improve the surgical outcome. Plantar heel pain may occur for multiple reasons and release of the lateral plantar nerve branch may be performed alongside the plantar fasciotomy in select cases. Possible complications of plantar fasciotomy include nerve injury, instability of the medial longitudinal arch of the foot, fracture of the calcaneus, prolonged recovery time, infection, rupture of the plantar fascia, and failure to improve the pain. Coblation (TOPAZ) surgery has recently been proposed as alternative surgical approaches for the treatment of recalcitrant plantar fasciitis.
Stretching Exercises
Stretching exercises for your foot are important. Do the stretches shown here at least twice a day. Don't bounce when you stretch. Plantar fascia stretch. To do the plantar fascia stretch, stand straight with your hands against a wall and your injured leg slightly behind your other leg. Keeping your heels flat on the floor, slowly bend both knees. You should feel the stretch in the lower part of your leg. Hold the stretch for 10 to 15 seconds. Repeat the stretch 6 to 8 times. Calf stretch. Stand with your hands against a wall and your injured leg behind your other leg. With your injured leg straight, your heel flat on the floor and your foot pointed straight ahead, lean slowly forward, bending the other leg. You should feel the stretch in the middle of your calf. Hold the stretch for 10 to 15 seconds. Repeat the stretch 6 to 8 times. Other exercises. You can also strengthen your leg muscles by standing on the ball of your foot at the edge of a step and raising up as high as possible on your toes. Relax between toe raises and let your heel fall a little lower than the edge of the step. It's also helpful to strengthen the foot by grabbing a towel with your toes as if you are going to pick up the towel with your foot. Repeat this exercise several times a day.